The Next Wave of HIV/AIDS: Nigeria, Ethiopia, Russia, India, and China
ICA 2002-04 D
September 2002
National
Intelligence
Council
ICA 2002-04D
The Next Wave of HIV/AIDS:
Nigeria, Ethiopia, Russia, India, and China
Prepared under the auspices of David F. Gordon, formerly
National Intelligence Officer for Economics and Global Issues.
Additional copies of this assessment can be downloaded from
the NIC public website at www.odci.gov/nic or obtained from
Karen Monaghan, Acting National Intelligence Officer for
Economics and Global Issues.
September 2002
Scope Note
This Intelligence Community Assessment (ICA) highlights the rising HIV/AIDS problem through 2010 in five countries of strategic importance to the United States that have large populations at risk for HIV infection: Nigeria, Ethiopia, Russia, India, and China. The paper does not attempt to make aggregate projections about global trends. The five countries were selected
because they are:· Among the world’s most populous countries, together representing over 40 percent of the world population.
· In the early-to-mid-stages of an HIV/AIDS epidemic.
· Led by governments that have not yet given the issue the sustained high priority that has been key to stemming the tide of the disease in other countries.
This paper builds on the December 1999 unclassified National Intelligence Estimate, The Global Infectious Disease Threat and Its Implications for the United States, which focused on the spread of AIDS in the context of other growing infectious diseases. Excerpts from the 1999 Estimate presage the expansion of the HIV/AIDS epidemic beyond the geographic focal point of southern Africa:
Although infection and death rates for HIV/AIDS have slowed considerably in developed countries…the pandemic continues to spread in much of the developing world. Sub-Saharan Africa currently has the biggest regional burden, but the disease is spreading quickly in India, Russia, China, and much of the rest of Asia.
According to UNAIDS, Asia alone is likely to outstrip Sub-Saharan Africa in the absolute number of HIV carriers by 2010.
The National Intelligence Council (NIC) convened a conference of US Government officials and outside experts to share their current assessments and expectations for the future of the disease in these five countries. Given the range of estimates of the current numbers of infected people and the lack of consensus on which infectious disease models calculate future rates most accurately, the future projections in this paper represent consensus estimates by experts. The NIC, in addition to coordinating the draft within the Intelligence Community, had the paper reviewed by several leading experts from outside the Intelligence Community as part of its effort to seek out expertise from inside and outside the government. The experts included Dr. Anthony Fauci, Director of the National Institute of Allergy and Infectious Diseases at the National Institutes of Health; Dr. Robert C. Gallo, Director of the Institute of Human Virology and Professor of Medicine at the University of Maryland Biotechnology Institute; Dr. Phillip Nieburg, Associate Director for Public Health Practice in the Global AIDS Program for the Centers for Disease Control; and Dr. Nicholas Eberstadt of the American Enterprise Institute.
Contents
Page
Scope Note
1
Summary
4
Discussion
7
The Scope of the Next Wave
Country Profiles
7
9
Prospects for Control
The Leadership Challenge
Weak Healthcare Infrastructure
Treatment
16
17
20
21
Implications
Nigeria and Ethiopia: Hardest Hit
Russia: HIV/AIDS Worsening Demographic Situation
India and China: A Big Problem But Probably Not Devastating
International Implications
22
22
24
24
26
Summary
The Next Wave of HIV/AIDS:
Nigeria, Ethiopia, Russia, India, and China
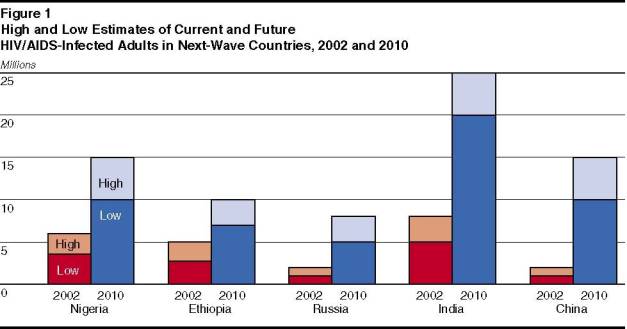
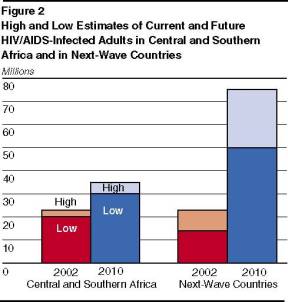
The number of people with HIV/AIDS will grow significantly by the end of the decade. The increase will be driven by the spread of the disease in five populous countries—Nigeria, Ethiopia, Russia, India, and China—where the number of infected people will grow from around 14 to 23 million currently to an estimated 50 to 75 million by 2010.[1] This estimate eclipses the projected 30 to 35 million cases by the end of the decade in central and southern Africa, the current focal point of the pandemic.
· We project China will have 10 to 15 million HIV/AIDS cases, and India is likely to have 20 to 25 million by 2010—the highest estimate for any country. By 2010, we project Nigeria will have 10 to 15 million cases, Ethiopia 7 to 10 million, and Russia 5 to 8 million.
HIV/AIDS is spreading at different rates in the five countries, with the epidemic the most advanced in Nigeria and Ethiopia. In all countries, however, risky sexual behaviors are driving infection rates upward at a precipitous rate.
· Adult prevalence rates—the total number of people infected as a percentage of the adult population—are substantially lower in Russia, India, and China, where the disease remains concentrated in high-risk groups, such as intravenous drug users in Russia and people selling blood plasma in China, where some villages have reported 60 percent infection rates.
· Nevertheless, the disease is spreading to wider circles through heterosexual transmission in India, the movement of infected migrant workers in China, and frequent prison amnesty releases of large numbers of infected prison inmates and rising prostitution in Russia.
It will be difficult for any of the five countries to check their epidemics by 2010 without dramatic shifts in priorities. The disease has built up significant momentum, health services are inadequate, and the cost of education and treatment programs will be overwhelming. Government leaders will have trouble maintaining a priority on HIV/AIDS—which has been key to stemming the disease in Uganda, Thailand, and Brazil—because of other pressing issues and the lack of AIDS advocacy groups.
· The governments of Nigeria, India, and China are beginning to focus more attention on the HIV/AIDS threat.
· Even if the five next-wave countries devote more resources to HIV/AIDS programs, implementation is likely to miss significant portions of the population, given weak or limited government institutions and uneven coordination between local and national levels.
· Nigeria and Ethiopia have very limited public services to mobilize. Russia is beset by other major public health problems. China has decentralized most responsibility for health and education issues to local governments that often are corrupt.
· India has taken some steps to improve its healthcare infrastructure to combat HIV/AIDS, but the government has few resources to treat existing infections and must cope with other major health problems such as tuberculosis (TB), which has become linked to the spread of HIV/AIDS.
The rise of HIV/AIDS in the next-wave countries is likely to have significant economic, social, political, and military implications. The impact will vary substantially among the five countries, however, because of differences among them in the development of the disease, likely government responses, available resources, and demographic profiles.
· Nigeria and Ethiopia will be the hardest hit, with the social and economic impact similar to that in the hardest hit countries in southern and central Africa—decimating key government and business elites, undermining growth, and discouraging foreign investment. Both countries are key to regional stability, and the rise in HIV/AIDS will strain their governments.
· In Russia, the rise in HIV/AIDS will exacerbate the population decline and severe health problems already plaguing the country, creating even greater difficulty for Russia to rebound economically. These trends may spark tensions over spending priorities and sharpen military manpower shortages.
· HIV/AIDS will drive up social and healthcare costs in India and China, but the broader economic and political impact is likely to be readily absorbed by the huge populations of these countries. We do not believe the disease will pose a fundamental threat through 2010 to their status as major regional players, but it will add to the complex problems faced by their leaders. The more HIV/AIDS spreads among young, educated, urban populations, the greater the economic cost of the disease will be for these countries, given the impact on, and the need for, skilled labor.
The growing AIDS problem in the next-wave countries probably will spark calls for more financial and technical support from donor countries. It may lead to growing tensions over how to disburse international funds, such as the Global Fund for AIDS, TB and Malaria.
The cost of antiretroviral drugs—which can prolong the lives of infected people—has plunged in recent years but still may be prohibitively high for populous, low-income countries. More importantly, the drug costs are only a portion of HIV/AIDS treatment costs. Drug-resistant strains are likely to spread because of the inconsistent use of antiretroviral therapies and the manufacture overseas of unregulated, substandard drugs.
· If an effective vaccine is developed in the coming years, Western governments and pharmaceutical companies will come under intense pressure to make it widely available.
· The next-wave countries are likely to seek greater US technical assistance in tracking and combating the disease.
HIV Statistics: Official and Unofficial Estimates
Reliable statistics on HIV/AIDS are difficult or impossible to get for many countries. UNAIDS maintains the most comprehensive databases of information in the world on AIDS, but the UN organization relies on official government statistics from each country—which experts believe sometimes understate the number of infected people. Our estimates of infection rates and their likely trajectories go beyond the official statistics by incorporating the assessments of academics and NGOs with field experience. As a result, all of the numbers in this assessment should be viewed as rough estimates, and our projections employ ranges to convey the general magnitude of the disease within a relatively high margin of error.
Governments often do not spend enough money to get quality infection surveillance because they have other budget priorities, do not want to acknowledge the extent of the epidemic, and the drug users and prostitutes at high risk of infection are not key political constituencies.
· Other hidden pockets of infection include TB patients—some of whom have contracted TB because they are HIV positive—and patients with venereal diseases and reproductive tract
infections.· It is difficult to get data on HIV prevalence rates in foreign military ranks, which harbor significant numbers of infected men.
Even if testing is available, many people do not get tested because of denial, stigma, discrimination, or resignation.
· Intravenous drug users, prostitutes, and homosexuals usually are reluctant to identify themselves for fear of punishment.
· Some avoid testing when healthcare and treatment for the disease is unavailable.
Infection surveillance of women attending prenatal clinics is considered the most reliable indicator of adult HIV prevalence in the general population. But even these statistics can be affected by poor clinic attendance when fee for services or mandatory HIV testing is instituted.
Discussion
The Next Wave of HIV/AIDS: Nigeria, Ethiopia, Russia, India, and China
The Scope of the Next Wave
The HIV/AIDS pandemic continues to spread around the world at an alarming rate, and the number of people with the disease will grow significantly by the end of the decade, as it becomes more geographically diffuse. By 2010, we estimate that five countries of strategic importance to the United States—Nigeria, Ethiopia, Russia, India, and China—collectively will have the largest number of HIV/AIDS cases on earth (see figure 1). These five countries, which comprise over 40 percent of the world’s population, are in the early-to-mid-stages of the epidemic.
· All five countries are major regional or global players, and efforts to manage the growing AIDS problem have the potential to impinge upon their political and economic outlook.
· The disease also is a special cause for concern in these five states because their governments have yet to demonstrate the kind of sustained commitment that has been key to managing the spread of HIV/AIDS in such countries as Uganda, Thailand, and Brazil.
We project the total number of people with HIV/AIDS in these "next-wave" countries is likely to soar from 14 to 23 million currently to 50 to 75 million by 2010, eclipsing the projected 30 to 35 million cases in central and southern Africa, the current geographic epicenter of the epidemic (see figure 2).
Through 2010, HIV/AIDS will increase more slowly or even decline in southern and central
Table 1
Current
2010
Current and Projected HIV/AIDS Infected Adults
Number
Infected
(Government Data)
(millions)Number
Infected
(Expert
Estimates)
(millions)Adult
Prevalence
Rate 2002*
(percent)Number
Infected(Expert
Estimates)
(millions)Adult
Prevalence Rate
2010*
(percent)Nigeria
3.50
4 – 6
6.00 – 10.00
10 – 15
18 – 26
Ethiopia
2.70
3 – 5
10.00 – 18.00
7 – 10
19 – 27
Russia
0.18
1 – 2
1.30 – 2.50
5 – 8
6 – 11
India
4.00
5 – 8
0.90 – 1.40
20 – 25
3 – 4
China
0.80
1 – 2
0.14 – 0.27
10 – 15
1.3 – 2
*Estimates of percent are based on population data from the US Bureau of the Census.
Africa—now in the sixth decade of the disease.[2]
· HIV adult prevalence [3] in central and southern Africa currently is the highest in the world. For example, as of July 2002, UNAIDS estimated that 39 percent of adults in Botswana (300,000 people) and 20 percent of adults in South Africa (4.7 million people) were HIV positive.
Although current adult prevalence rates in the next-wave countries range from less than one percent in China to as high as 18 percent in Ethiopia, the number of people infected already is substantial, ranging from 1 to 2 million in China and Russia to upwards of 5 million in Nigeria and India (see table 1).
The spread of HIV/AIDS in the next-wave countries will be difficult to check by 2010. Treatment of existing infections and prevention of new infections is minimal. Even if effective programs could be implemented in the coming years, such practical concerns as cost, scale, and experience in health service delivery probably will result in the omission of services to a large number of infected individuals, and the burden of disease will continue to rise.
· We project that China probably will have 10 to 15 million HIV/AIDS cases by 2010. India is likely to have 20 to 25 million—higher than projected for any other country. We estimate Nigeria probably will have 10 to15 million cases, Russia 5 to 8 million, and Ethiopia 7 to 10 million.
Country Profiles
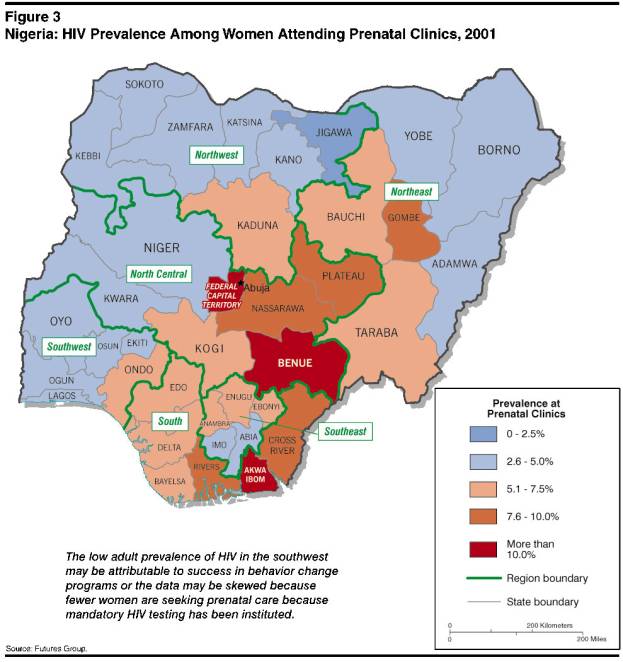
Nigeria. The HIV/AIDS epidemic in Nigeria is significantly ahead of that in India, China, and Russia—already advancing well beyond high-risk groups and into the general population. The official adult prevalence rate is almost 6 percent, but unofficial estimates range as high as 10 percent—which represents 4 to 6 million people infected.
Heterosexual transmission of the HIV virus is the primary mode of spread in Nigeria, and infections appear to be as numerous in rural areas as in the cities. The reported rate of infection apparently varies significantly by region, with the lowest reported rate found generally in the predominantly Muslim northern parts of the country (see
figure 3). Infections are most numerous among men ages 20 through 24, but some experts caution that infection rates are rising quickly in young women.
Given the already advanced state of the disease and the government’s limited capacity to respond, we expect HIV/AIDS to infect as many as 10 to 15 million people by 2010. This number would constitute roughly 18 to 26 percent of adults—close to the current rates in some of the hardest hit countries in southern Africa.
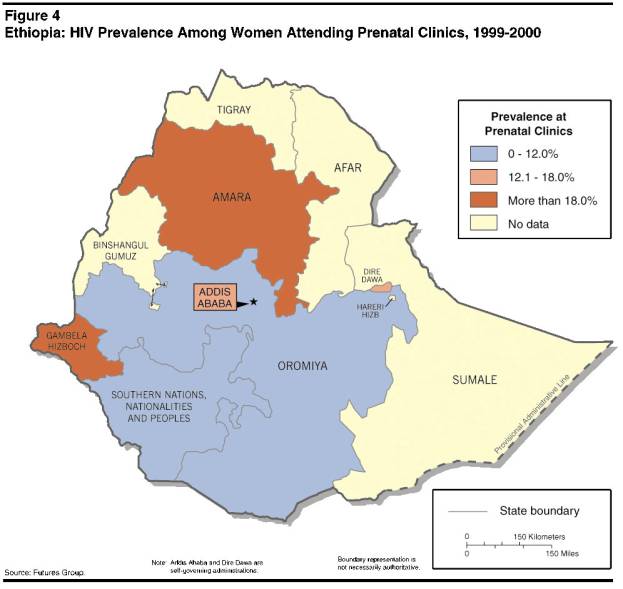
Ethiopia. Ethiopia’s adult prevalence rate—estimated at between 10 and 18 percent—is the highest among the five countries, indicating that—like Nigeria—the disease has moved significantly into the general population. Government figures cite 2.7 million Ethiopians currently as HIV positive, although experts believe the actual number may be between 3 and 5 million. Adult prevalence is much higher in cities (13 to 20 percent) than in rural areas (5 percent) (see figure 4). The generally poor health of Ethiopians as a result of drought, malnutrition, limited healthcare, and other infectious diseases has caused HIV to progress rapidly to AIDS. Heterosexual transmission is the primary mode of spread, and people with multiple partners—especially those with sexually transmitted diseases (STDs) and prostitutes—have significantly higher infection rates, ranging from 30 to 40 percent in STD-positive individuals to 50 to 70 percent in prostitutes.
Unlike conditions in other next-wave countries, war has significantly contributed to the spread of the disease in Ethiopia. Many soldiers contracted HIV/AIDS during the civil war in the 1980s by having contact with multiple sex partners. When the war ended in 1991, thousands of infected soldiers and prostitutes returned home, spreading HIV/AIDS in their villages and towns.
· Another surge of infections may be underway. Ethiopia has demobilized 150,000 soldiers over the last two years as the conflict with Eritrea has wound down. More troops will be sent home as the border dispute is settled.
· As soldiers demobilize, prostitutes—who have even higher rates of infection—disperse around the country as well.
Looking ahead, we expect 7 to 10 million Ethiopians probably will be infected by 2010 because of the high current rate of adult prevalence, widespread poverty, low educational levels, and the government’s limited capacity to respond more actively.
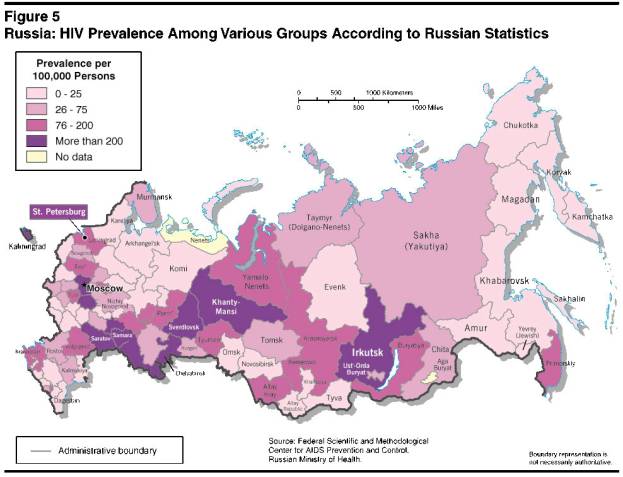
Russia. Official statistics list about 200,000 people in Russia as HIV positive, but the government’s sampling efforts are poor, especially outside major cities. Academic and medical experts believe the actual number probably is between 1 and 2 million, which would indicate an adult prevalence rate of around 1 to 2 percent.
· Infection rates vary significantly across the country, with the biggest concentrations in cities (see figure 5). Males comprise 77 percent of all the infected, and 60 percent of infected men are between the ages of 17 and 25.
Intravenous drug use drives the spread of the disease in Russia more than in any of the other next-wave countries. An estimated 80 to 90 percent of all infections in Russia stem from intravenous drug use, which is rampant and rising.
· In most countries, the concentration of HIV among drug users and generally low adult prevalence rates would suggest the disease still has not broken out into the general population. Experts warn, however, that drug use is so widespread in Russia that many users are integrated into society with jobs and families, suggesting the disease is moving into the mainstream.
Prostitutes and prison inmates—many of whom are intravenous drug users—are contributing to the spread of the disease. An estimated 20 to 25 percent of intravenous drug users in prison, where there is easy access to drugs, are HIV positive.
· Russia’s frequent use of prison amnesty programs that release infected inmates will worsen the HIV/AIDS epidemic among the general population unless accompanied by prevention and treatment programs.
· The growing number of prisoners infected with both HIV and tuberculosis is compounding the burden; HIV infection increases the likelihood that a person with TB will develop the active, contagious form of TB.
· Moreover, laws allowing the incarceration of suspects for up to two years prior to be-ing charged create a revolving door of inmates who often are intravenous drug users infected with TB and/or HIV.
HIV/AIDS also is a growing problem in the Russian military services. Currently up to one-third of prospective conscripts are deemed unfit for service owing to the effects of prior drug use (chronic hepatitis or HIV infection). Amongst enlisted men, ground troops have the largest number of infections, while strategic military forces and airborne troops have the lowest.
Driven by widespread drug use, inadequate healthcare infrastructure, and the government’s limited capability to respond, the number of HIV positive people probably will rise to 5 to 8 million by 2010. This condition would reflect an adult prevalence rate of around 6 to 11 percent, exacerbating Russia’s population decline.
India. According to official Indian Government statistics, 4 million people in India are HIV positive. India also has high rates of TB, however, which may be indicative of undiagnosed HIV/AIDS. Some experts believe that 5 to 8 million Indians may be infected. We
expect India to have the largest number of people with HIV/AIDS in the world within the next few years. But even with the large number of infected people, India’s adult prevalence rate is only around one percent.
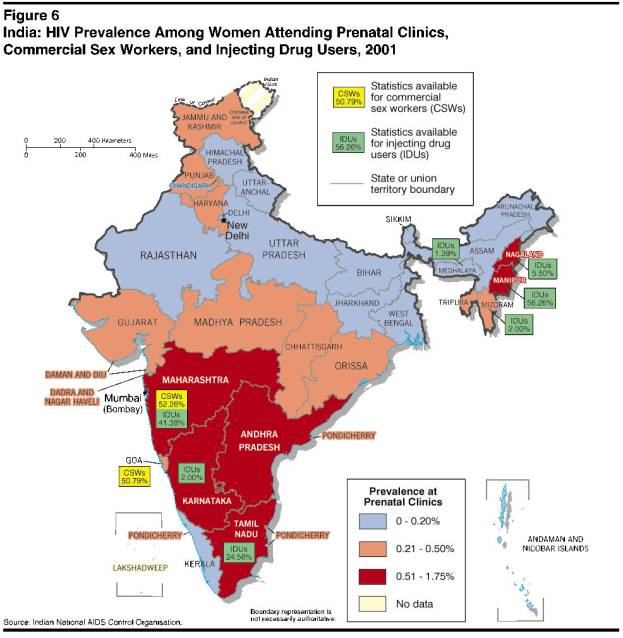
· Adult prevalence rates vary across the country, however, in some areas (Mumbai and Pune) the rate is as high as 4 percent, according to unofficial estimates
(see figure 6).Heterosexual transmission is the driver of infections, except in two regions (Nagaland and Manipur) where intravenous drug use is a serious problem. Thirty to 60 percent of prostitutes and up to 15 percent of all truck drivers are infected with HIV/AIDS.
· Sexually transmitted diseases and reproductive tract infections are rampant in India, increasing the risk that HIV/AIDS infections will be transmitted.
The current trajectory of the disease, limited public awareness, and the lack of resources for a major anti-AIDS program will continue to drive the spread of the disease. Approximately 20 to 25 million Indians are likely to be infected by 2010—even if the disease does not break out significantly into the mainstream population.
China. China has significantly raised its official estimate of the number of HIV-positive people over the last two years from 600,000 to one million. The UN now estimates that 1.5 million are infected, while other experts believe the number probably is closer to 2 million or even higher. Owing to China’s massive population, even these higher figures, however, represent an adult prevalence rate of only 0.15 to 0.25 percent.
HIV: The Science of the Disease
HIV-1 is a fatal infection acquired by contact with the blood or body fluids of an infected person. A transfusion with infected blood almost always results in spread of the virus, and children born to infected mothers have an up to 40 percent chance of contracting the virus—prior to birth, during birth, or through breastfeeding. The transmission rate of the disease through sexual contact ranges from 1 to 3 percent. Reusing infected needles results in infections less than one percent of the time.
Sexually transmitted diseases or reproductive tract infections greatly increase the risk of contracting HIV, and uncircumcised men transmit HIV and other STDs to their partners more frequently than circumcised men.
As the disease progresses, a type of infection-fighting white blood cell—the CD4 positive-t cell—decreases, leading to an irreversible loss of immune function. This period is marked by many illnesses, or unusual “opportunistic” infections that healthy immune systems protect against.
HIV-positive persons are susceptible to opportunistic and infectious diseases, especially TB. Once they have contracted TB, the disease progresses to the highly infectious, active stage much more quickly and frequently than in HIV-negative persons and is often what kills them.
Antimicrobial medications are used to treat opportunistic infections of bacterial, viral, and fungal origin. Frequent or prolonged use of antimicrobials promotes genetic mutations that result in drug resistance. This often makes opportunistic infections more serious and difficult to treat, and may drive the spread of resistant organisms in both HIV-positive and HIV-negative people.
Antiretroviral and other antimicrobial medications can prolong life, but eventually the immune system becomes so damaged that HIV progresses to Acquired Immune Deficiency Syndrome (AIDS), and death usually follows in a few years. No cure for HIV/AIDS is available, and no vaccine has proven a sure way to prevent it; avoidance of high-risk behavior is the only proven way to prevent the disease.
A generally milder form of the virus (HIV-2) also exists and has limited geographic reach—primarily in West Africa, including Nigeria—and is less transmissible and less lethal than
HIV-1. Patients with HIV-2 have lower viral loads and slower immune decay but acquire the same opportunistic infections as those infected with HIV-1.
Several factors are driving the epidemic in China—the large migrant population, intravenous drug use, and poor hygiene in plasma sales—increasing the odds that the disease will continue to spread.
Migration. An estimated 100 million ruralmigrants are on the move in China, relocating to cities to find work. Sexual contact between migrant men and prostitutes has spread the disease, which advances over an even wider geographic area if the migrants return to their villages to visit their families.
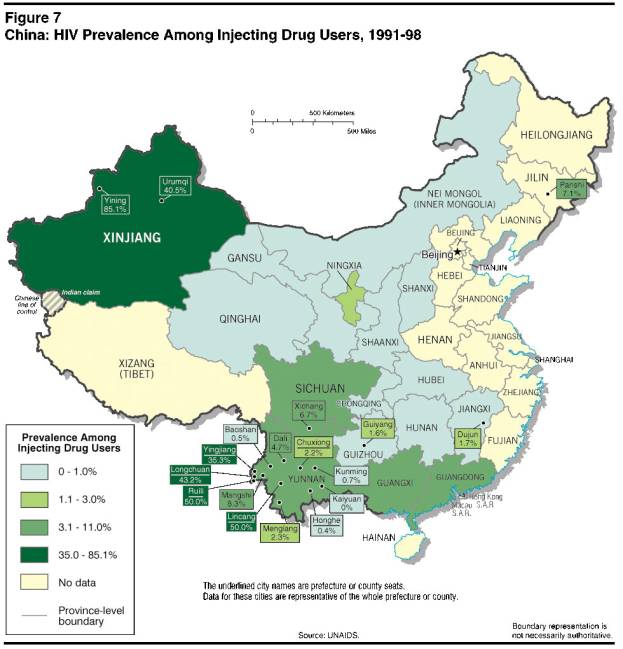
Drug abuse. HIV/AIDS also is rising among intravenous drug users, especially in southern regions adjacent to Southeast Asia’s “GoldenTriangle” of heroin production and distribution routes. Infection rates also soar as high as 85 percent among intravenous drug users in the Xinjiang Autonomous Region in western China (see figure 7).
Plasma sales. The practice of plasma selling in rural areas also has been a major contributor to the spread of HIV/AIDS (see textbox). Mixing infected blood plasma causes one of the highest known transmission rates for HIV/AIDS, and the practice has infected large numbers of rural, heterosexual villagers who would otherwise be considered at low risk for the disease.
Despite growing concern over the disease among senior leaders, China’s sheer size, resource constraints, widespread ignorance of AIDS, cultural taboos about discussing sex, and coordination problems between levels of government will make it difficult to check the spread of the disease.
· Even if adult prevalence rates rose only to two percent by the end of the decade, China would have about 15 million infected people by 2010—surpassed only by India.
Prospects for Control
We assess that all five next-wave countries will have difficulty controlling their HIV epidemics in the short to medium-term. The disease has built up significant momentum—especially in Nigeria and Ethiopia—and the governments have been slow to respond. None of the five next-wave countries in this report is on a trajectory to replicate the success of such countries as Uganda, Thailand, and Brazil in stemming the spread of the disease. Several leaders of the next-wave countries are focusing more attention on the AIDS threat, but all face a host of competing demands. In addition, these countries have weak healthcare infrastructures and severe budget constraints, which will create difficulty in financing education and treatment programs for their large populations.
China: HIV Infections from Blood Selling
Most of China’s blood supply is purchased from poor villagers by brokers who collect only plasma for the manufacture of therapeutic and diagnostic products. These brokers often try to save money and time by mixing the blood of several donors before spinning out the plasma in a centrifuge. Reinjecting the mixed blood back into the donors to prevent anemia has spread HIV like wildfire, with infection rates as high as 60 percent in some villages. The government has
ordered a stop to the practice, but press reports suggest that it continues in some areas. The practice of blood selling began as a way to raise money for rural health projects after the central government cut subsidies to the provinces.· Chinese media report that people selling blood in Qinghai, Henan, and Shaanxi claim that they earn between $12 and $15 for each bag of donated blood—a large sum of money in these poor provinces. Some farmers report donating blood 50 times in two months.
The high cost and complexity of treatment programs probably will continue to feed the debate over the relative cost/benefit of treatment versus prevention in addressing HIV/AIDS.
· Pressure for antiretroviral drugs has jumped in recent years because such drugs afford one of the most tangible ways for governments to respond to the AIDS problem.
· Nonetheless, successful efforts to combat HIV in Uganda, Thailand, and other countries suggest that high-profile education programs to change behaviors remain key to long-term success, although this approach requires more time and persistence by senior leaders.
The Leadership Challenge
The commitment of senior political leadership to persist in the struggle against HIV/AIDS has been a key variable in the few successful programs around the world. The leaders of Nigeria, Ethiopia, Russia, India, and China will be challenged to maintain sustained high-level interest, however, given the scope and severity of other domestic and foreign policy issues. Some leaders are beginning to pay more attention to AIDS, but they have not given it the sustained priority thus far that has been needed in other countries to blunt the spread of the disease.
Overcoming Social Stigmas
Many citizens and government officials in next-wave countries are reluctant to acknowledge the spread of the disease owing to strong social and cultural norms. HIV/AIDS still is associated with behaviors widely considered taboo, including prostitution, drug use, and homosexuality. HIV-positive people often do not seek testing and treatment because they fear being ostracized by their families, neighbors and friends and losing their jobs or access to public services.
· In China, few people publicly acknowledge HIV-positive status because they might be barred from school, fired from their jobs, or even expelled from their community, according to press reports. Largely as a result of China’s “one-child” policy to reduce population growth, Chinese men are under such pressure to carry on family lines that some HIV-infected gay men marry and have families and risk spreading the disease to their wives and children.
· A 2001 law in one Chinese province prohibits HIV-infected persons from marrying.
· In India, recent studies found that HIV-infected people were refused admission to some hospitals and denied treatment. Furthermore, HIV test results often are not kept confidential, which discourages people from getting tested. Some experts say that women in India’s male-dominated society are reluctant to insist on condom use, and the widows of men who die from AIDS sometimes are denied healthcare or contact with their children.
HIV/AIDS: Success Stories to Model
Uganda, Thailand, and Brazil have managed the spread of HIV largely through active, high-level leadership to increase awareness, destigmatize the disease, and treat victims—all of which help change the behaviors that transmit the disease. These countries are widely considered to have the most successful anti-HIV programs and are potential models for other countries ravaged by the disease.
· Bold leadership by Uganda’s President Museveni largely is responsible for driving down the country’s infection rate from 30 percent in 1992 to 11 percent in 2000. The HIV/AIDS problem remains significant, but Museveni has had success in his relentless campaign to change behavior by urging people not to have sex with multiple partners, publicly acknowledging the threat posed by AIDS, destigmatizing the disease, and decentralizing HIV education programs down to the village level.
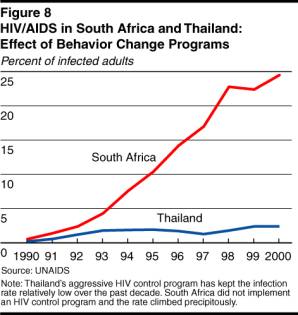
· Thailand launched a massive HIV/AIDS public awareness and condom distribution campaign in the early 1990s—with the support of several key senior officials—which significantly reduced the spread of the disease. More recently, the government announced it would make antiretroviral drugs available for less than one dollar a day. AIDS still is the leading cause of death in Thailand, but the government probably has averted millions of HIV infections (see figure 8).
· In Brazil, the government has invested heavily in education and treatment programs, including providing free antiretroviral drugs to HIV/AIDS patients distributed through the public health system. HIV adult infection prevalence also is declining among intravenous drug users, suggesting that programs teaching safer injection habits also are successful.
Active leadership will be especially critical given the widespread public ignorance of AIDS in next-wave countries. The challenge is especially great in these countries because of fragile communications links, numerous government jurisdictions, and different ethnic and language groups. The five countries also lack strong domestic advocacy groups that can raise awareness and increase pressure for responsive programs.
· A survey two years ago found that 20 percent of Chinese respondents had never heard of HIV/AIDS, and over 60 percent did not know how the disease spreads or how to prevent infection.
· A World Bank study in India indicates that public awareness of the disease and condom use remain low despite government education programs.
· In Nigeria, a healthcare worker was
fired after she tested positive for HIV, although a court ultimately agreed to hear her appeal.· Russia appears to be a major exception. A survey last year by an independent pollster found that 90 percent of those polled see combating HIV/AIDS as an important issue.
Nigeria’s leadership has been the most active of the five countries in trying to raise AIDS awareness, for example, by hosting a regional AIDS conference in 2000 and publicly warning about the risk of “extinction” on the continent. Nonetheless, the Obasanjo administration is beset by such other pressing problems as an approaching election and rising ethnic and religious tensions. Moreover, Nigeria’s government institutions have deteriorated so badly over the last decade that Obasanjo has few functioning public sector assets left to mobilize even if he chose to engage fully on the issue.
· Nigeria has taken some steps, however, to build domestic monitoring and diagnostic capabilities—especially in Lagos—and a major study on the economic effects of HIV/AIDS is underway.
· The Nigerian military, concerned about the loss of key personnel from AIDS, now mandates training about the disease for soldiers.
The Ethiopian Government does not appear focused on AIDS, despite occasional statements on the issue. The government has focused in recent years on the conflict with Eritrea. Healthcare workers privately have criticized efforts in recent years as half hearted, and UN officials have publicly warned Ethiopian leaders to take more measures to stem the epidemic.
The Russian Government has not mounted a sustained effort up to now to publicize the growing threat of HIV/AIDS. Russia faces so many other serious problems that HIV/AIDS is unlikely to receive high-level attention for an extended period until the economic and security costs of neglect become more
tangible.
· In 2001, Moscow promised $133 million to fight AIDS over five years, but it has only appropriated $80 million ($16 mil-lion per year). Treating 3 million HIV- infected adults would cost $30 billion a year, according Vadim Pokrovsky, the chief of the Russian Federal AIDS Center.
· In 2001, Moscow refused a World Bank loan to fight TB and HIV/AIDS, apparently because Russia did not wish to increase the amount of its debt. However, Moscow recently re-opened negotiations for the loan.
The Indian Government has taken numerous steps to highlight the risk that AIDS poses to the country, but tensions with Pakistan and growing religious strife clearly are considered more pressing issues. Furthermore, India faces competing priorities to address such other health challenges as TB. Nonetheless, the Indian Government did react to the emergence of HIV/AIDS in 1986 by creating the National AIDS Control Organization (NACO).
· NACO faced many difficulties throughout most of its early years, although new leadership in 1999 has improved and expanded the HIV/AIDS program.
The Chinese Government has become significantly more open over the last year in acknowledging the rising HIV/AIDS problem after ignoring it for years. The central government has organized some public relations events to increase awareness of the disease, and Beijing has sought bilateral assistance from the United States and others to improve its anti-AIDS campaign.
· A Chinese government official has publicly expressed concern that there could be 10 million people with AIDS by the end of the decade.
· The turnaround suggests that senior leaders are concerned about the potential economic, social, and political ramifications of the spreading disease.
Nonetheless, domestic funding to combat the disease remains low, and Chinese leaders will have difficulty keeping HIV/AIDS high on the agenda as they struggle to deal with such challenges as maintaining economic growth, defusing rural discontent, managing the Communist Party leadership transition, opening Chinese markets more widely to trade, and modernizing the military. Moreover,
decisionmaking has become so decentralized in China on healthcare and education that senior leaders in Beijing cannot always count on provincial and local leaders to follow through.· Local government commitment to HIV/AIDS is likely to be uneven, given the low funding for such programs from the central government, lack of awareness of the disease, stigmatization of those infected, and corruption.
· Some government leaders probably will be especially reluctant to highlight HIV/AIDS because they may be linked to the blood selling programs that have become a major means of transmission.
· In July 2002, Chinese police detained for several months the country’s most prominent AIDS activist for circulating a “secret” government memo acknowledging that poor management of the blood supply had contributed to the AIDS problem.
Weak Healthcare Infrastructure
Although significant differences in capabilities exist among next-wave countries, all five have overburdened and under funded healthcare systems and limited abilities to provide integrated, nationwide programs to test people, track infections, and deliver treatment and education programs. Even within each of the five next-wave countries there are disparities in the ability of cities and regions to deal with the epidemic that are likely to grow in the coming years.
· Nigeria’s public healthcare system, which has been deteriorating for years, is hard pressed to provide even the most basic public services. Many facilities lack electricity, water, and soap; even better-equipped hospitals are beset by strikes by medical staff.
· Ethiopia has never had a viable national healthcare system because of overwhelming poverty and years of war. The government is soliciting international assistance to build its capabilities, but progress on this front is likely to take years.
· Russia’s dwindling health services are unable to provide treatment for many victims of heart disease and the skyrocketing number of TB cases. Since the breakup of the Soviet Union, Russia’s health infrastructure has deteriorated so much that most experts believe that the population is less healthy now than at any time in the past 50 years.
· India has established nationwide HIV/AIDS centers and a monitoring system, but access to basic medical care is not universal and the free public health- care system often is highly inefficient. Nonetheless, the government’s AIDS organization was able to reach an estimated 70 percent of households in a recent survey of AIDS-related behavior.
· In China, a growing number of citizens cannot afford quality healthcare because of privatization of the public health service. Rural areas, which have the highest HIV infection rates and where 70 percent of the population lives, suffer from major shortages of resources. Funds are being directed toward modernizing urban facilities.
Treatment
Brazil’s successful emphasis on treatment and the expanded use of antiretroviral drugs has raised hopes for improving the length and quality of life for HIV/AIDS patients. Nonetheless, we believe treatment will be a
Antiretroviral Drug Resistance
Natural viral mutation and improper use of drugs to control HIV (halting use, intermittent use, or habitually missed doses) have caused some strains of HIV to evolve resistance to antiretroviral medications. These resistant strains continue to reproduce and destroy immunity in the presence of medications meant to control the virus, and already they have spread around the world. These drug-resistant variants are spread less efficiently than other forms.
· HIV strains have an amazing ability to recombine to form mosaic viruses. This pace of genetic change forces changes in treatment regimens and has placed unprecedented pressure on the pharmaceutical industry to develop new drugs for continued viral control.
· Most HIV drug resistance can be traced to improper use of medications. Weak healthcare infrastructures in some next-wave countries will lead to poor distribution and incorrect use of antiretrovirals, which are likely to promote drug resistant strains of HIV and reduce the effectiveness of medicines.
· Treatment failure rates can be as high as 60 percent in some countries.
To help control resistance, therapies now often employ a combination of several drugs from different classes. In addition, some researchers are now trying to curb the growth of antiretroviral resistance by having medical workers personally watch and record patients taking medication—known as direct observed therapy—a technique that has slowed the development of resistance to anti-TB medications.
· Important new drugs inhibiting viral entry into healthy cells also are in development, but prohibitive costs are likely to limit their distribution in the developing world.
difficult primary strategy for the next-wave countries because of the high cost of providing antiretroviral drugs for such large populations and drug resistance.
· The cost of antiretroviral drugs has plunged in recent years—from around $10,000 per year per patient down to as low as $500 to $600—because of pressure from many countries on pharmaceutical companies and the increasing use of generic drug alternatives.
· Pharmaceutical industries in an increasing number of countries—including Russia, India, and China—are likely
to develop and produce such drugs in
the interest of reducing the cost of
medication.· A Chinese government official publicly warned in September 2002 that Beijing would authorize domestic firms to manufacture generic drugs in defiance of patent laws unless prices come down, although the Ministry of Health later said it would not violate WTO obligations.
Even as prices decline, the total cost of providing drugs for millions of patients is likely to be prohibitively high for populous, low-income countries. Moreover, the cost of the drugs is only a small portion of the overall cost of treatment programs. Costly laboratory tests and equipment are needed to determine which combination of drugs is appropriate for each infected person.
· The effectiveness of the drug combinations must be monitored and adjusted on an ongoing basis as well.
The effectiveness of antiretroviral drugs also is being undermined by a growing drug resistance problem, owing both to the natural mutation of the virus and improper drug use.
· Weak HIV and TB treatment programs in Russian prisons will foster the emergence of drug-resistant strains, which eventually are likely to appear outside Russia because of growing international travel.
· Scientists at the July 2002 international AIDS conference in Barcelona presented numerous research papers on the challenge of drug resistance and the consequences of not taking medicines as
prescribed.Implications
The rise of HIV/AIDS will have significant economic, social, political, and military implications in Nigeria, Ethiopia, Russia, India, and China, although the percentage of the adult population in each country that is infected is likely to remain below the hardest hit countries in southern and central Africa. The impact of the disease by the end of the decade will vary among the five countries, given differences in disease trajectories government responses, available resources, and demographic profiles.
Nigeria and Ethiopia: Hardest Hit
The social and economic impact of AIDS in Nigeria and Ethiopia probably will be similar to the hardest hit countries in Africa. The disease is likely to negatively impact almost all sectors of society by 2010. AIDS will take a heavy economic toll by robbing the countries of many key government and business elites and by discouraging foreign investment, although the oil sector is unlikely to be hurt significantly.
· The professional classes in Nigeria and Ethiopia—like other African countries—are more vulnerable in comparison to other next-wave countries because adult prevalence rates already are much higher and relatively fewer elites are concentrated in a smaller number of key
positions.· The drag of AIDS on economic growth will further reduce the ability of the government to handle the rising social and healthcare costs.
The further deterioration of already weak government institutions by the escalating HIV/AIDS crisis could leave Nigeria and Ethiopia seriously weakened states and is likely to reduce their ability to continue to play a regional leadership role.
· HIV/AIDS probably will complicate staffing in the military officer corps of the two countries as it has in other African states. Ethiopia is more likely to suffer military manpower shortages through the lower ranks, however, because it has a much larger army and smaller population than Nigeria, which plans to reduce the size of its force.
· Rising social tensions over AIDS and related economic problems could exacerbate regional and ethnic tensions within Nigeria and Ethiopia while leaving both governments less able to manage the problem.
AIDS Vaccines Coming, But Not a Panacea
Many research and clinical trials are underway to develop a vaccine against HIV. Clinical trials of two commercial vaccines—intended to confer immunity by introducing a harmless portion of HIV protein into the body—have progressed to Phase III human testing in the United States, Canada, Netherlands, and Thailand. Results are expected within the year. Nonetheless, even if a viable vaccine to protect against certain viral subtypes of HIV that are prominent in the test countries becomes available in the coming years, it probably will not to be effective against the most common subtypes of HIV in Nigeria, Ethiopia, Russia, India, and China.
Moreover, first-generation HIV-vaccines probably would provide lower immunity or shorter-lived protection than future product iterations that incorporate what is learned from wider use. Studies suggest that if the vaccine is at least 30 percent effective, delivering it to persons engaging in high-risk behaviors may be beneficial, although there is a danger that it could encourage risky sexual conduct in individuals who believe they are protected by the vaccine. Unless the vaccine was widely affordable, however, it would remain beyond the reach of the developing world—which is likely to fuel intense political pressure on Western countries and drug companies to slash prices or subsidize the cost.
Both vaccine effectiveness and good distribution are necessary for HIV transmissibility to decrease enough for the epidemic to die out eventually. For example, some estimates indicate that to stem the epidemic, the world would need 50 percent coverage with a 75 percent effective vaccine. Until a highly effective vaccine is in wide distribution, anti-AIDS programs aimed at encouraging behavioral change will remain essential in controlling HIV/AIDS.
· If the governments prove unable to respond, public confidence in political leadership could be weakened further, especially if efforts to respond are seen to be undermined by corruption.
Researchers estimated there were 2.6 million AIDS orphans in Nigeria alone in 2000—higher even than in South Africa—and the problem will get much worse. AIDS orphans often are taken in by relatives during the early stages of the disease, but the phenomenon in other African countries suggests that Nigeria and Ethiopia are likely to reach a point before the end of the decade when the number of caregivers is insufficient to cope with the burden.
Russia: HIV/AIDS Worsening Demographic Situation
The rising AIDS problem in Russia is likely to exacerbate the significant social, economic, health, and military problems already facing the country. These challenges, added together, will complicate Moscow’s efforts to rebuild Russia.
· HIV/AIDS will accelerate Russia’s population decline. A contracting work force and exploding healthcare costs will be serious counterweights to energy-driven economic growth.
· A recent World Bank study projects that HIV/AIDS could cut annual economic growth in Russia by half a percentage point by 2010 and a full percentage point by 2020.
As the disease spreads, the high cost of treatment and education programs could drive out other claims on health systems, leading to a steeper decline in general health than caused by HIV/AIDS alone. Even if more resources are committed to combat HIV/AIDS—either by Russia or outsiders—considerable time and money would be required to expand and reform the healthcare infrastructure, suggesting that the disease will continue to spread at a rapid pace.
· These economic problems are likely to fuel social and political tensions over spending priorities. Devoting more money to combating HIV/AIDS probably would just leave that much less for such other pressing health problems such as heart disease and TB.
India and China: A Big Problem but Probably not Devastating
India and China are likely to generate the largest number of people infected with AIDS of any countries in the world by 2010, but the impact will be lessened because these individuals will remain diffused among very large populations. Even if the number of infected people rises to the upper side of our projections, the percentage of the adult population that is infected still would be significantly lower than in the other next-wave countries at the end of the decade.
· Fifteen million HIV-positive people in China would represent roughly 2 percent of the adult population.
· Twenty-five million infected Indians would reflect a 4 percent adult prevalence rate.
Judging the broader impact on economic growth and productivity is more difficult, however, because it depends largely on which demographic groups get hit the hardest. Several researchers in 1999 estimated that AIDS cost India roughly 1 percent of GDP per year because of lost productivity and treatment of secondary infections. The study did not include numerous factors—such as the cost of drugs and retraining workers—however, and there is no consensus on a formula to calculate the economic costs.[4]
· At a minimum, AIDS will drive up healthcare costs in both countries, forcing difficult trade-offs on spending.
· The more the disease remains among rural and lower skilled people, the more likely that the abundant labor supply of both China and India can fill the gap.
· The more the disease spreads among young, educated, urban professionals, however, the higher the economic costs will be, given the premium on skilled
labor.· Chinese leaders are likely to fear that the perception in global markets of a rising AIDS problem could discourage the huge flow of foreign investment into the country that has been vital to growth.
We believe the HIV/AIDS epidemic, by itself, will not pose a fundamental threat through 2010 to the rise of China and India as major regional players. Given the relatively low current prevalence rates and the relatively long period from infection to death, the two countries can manage the impact of the disease through the end of the decade. Nonetheless, the mounting AIDS problem will further add to the complex problems and trade-offs facing leaders in both countries in the coming years.
· Beyond 2010, HIV/AIDS will become an even more significant problem for China and India if government programs prove ineffective and prevalence rates jump significantly.
There is no sign that HIV/AIDS will become a lightning rod for widespread public discontent in either China or India. Nonetheless, the protests of rural Chinese who became infected through plasma sales suggest that anger with the government’s slow response will add to growing frustration in rural areas over rising unemployment, widespread corruption, and poor services.
· Press reports indicate that several small-scale AIDS-related protests have erupted in Chinese villages over the last year. Journalists report that many villagers
are angry over the issue but are afraid to speak out because of government
intimidation.· For several days in November, police detained HIV-positive protesters and a group of reporters who came to interview them.
· Protests by Chinese in urban areas almost certainly would spark deeper concern among Chinese authorities.
· HIV/AIDS may become more of a political issue in India as infection rates climb. The debate is likely to focus on who pays for and receives the antiretroviral drugs that Indian firms now are producing.
Both Beijing and New Delhi probably will try to push the rising cost of dealing with HIV/AIDS down to state and local governments, as they have on other issues. Local authorities, however, are unlikely to have the staff, expertise, or funding to assume the growing burden.
· Most Indian state governments already have curbed spending on healthcare and education to cope with severe fiscal strains—and some are even struggling just to pay the wages of government workers.
· Likewise, Chinese localities already are overburdened with responsibilities for public health that Beijing has passed along in decentralizing many government duties.
HIV/AIDS is unlikely to undermine general military capabilities in China and India because of the large pool of potential recruits for the respective armies. China began testing conscripts for HIV in 2001.
· China and India increasingly will monitor AIDS in the military to ensure that the disease does not complicate staffing among smaller, more highly trained units operating sophisticated weapon systems.
As HIV/AIDS moves more into the general population in China, past experience in other countries suggests it will exacerbate an already existing gender imbalance because of the practice of female infanticide.
· In India and China, because of cultural norms, boys are more likely to be taken care of by their relatives than girls.
International Implications
The surge in the disease outside southern Africa will fuel calls for more support from donor countries to address the problem and intensify the debate over how to allocate such international resources as the Global Fund for AIDS, TB, and Malaria.
· UN Secretary General Annan set a goal of raising international spending on AIDS to $7-10 billion a year when he proposed the Global Fund last year. Based on rising projections for the next-wave countries, pressure will grow to significantly raise that amount.
· A debate is likely over how much the Global Fund should focus on heading off AIDS in large, next-wave countries where it is in the earlier stages, and how much to devote to the hardest hit countries in southern Africa. Similarly, differences are likely to arise between those wanting to allocate money to programs on the basis of proven success or greatest need.
· Should resources be shifted away from central and southern Africa, Africans there probably will accuse the West of ignoring them and paying more attention to large countries that are more economically and strategically important.
The rising focus on HIV/AIDS worldwide has the potential to draw international attention and funding away from other infectious diseases such as TB, malaria, hepatitis, as well as other critical non-infectious health problems.
International tensions over medical treatment for HIV/AIDS almost certainly will grow, even though access to antiretrovirals will
increase.· The manufacture of generic antiretroviral drugs by several next-wave countries will increase pressure on international pharmaceutical companies to further lower the price and increase availability of their drugs. European countries have stated their support for countries buying AIDS drugs from companies in India and Brazil that challenge patents.
· The increasing use of antiretrovirals in next-wave countries, however, almost certainly will increase misuse due to their weak healthcare systems, undermining their effectiveness and fueling resistant HIV strains throughout the world. If the effectiveness of antiretrovirals declines, recipient countries are likely to charge donors with supplying faulty drugs.
· Developed countries will face overwhelming pressure to provide any new vaccines that are discovered to countries around the world. These countries will complain bitterly if the early vaccines are not designed for the HIV subtypes common in their regions or blame the donors for their limited effectiveness.
Despite these likely frictions, however, the rising AIDS crisis probably will make the next-wave countries more open to seeking technical assistance from the United States and other donor countries to help track, prevent, and treat the disease.
The National Intelligence Council
The National Intelligence Council (NIC) manages the Intelligence Community’s estimative process, incorporating the best available expertise inside and outside the government. It reports to the Director of Central Intelligence in his capacity as head of the US Intelligence Community and speaks authoritatively on substantive issues for the Community as a whole.
Acting Chairman
Stuart A. Cohen
Vice Chairman for Evaluation
Mark Lowenthal
Acting Director, Senior Review,
Production, and Analysis
William R. Heaton
National Intelligence Officers
Africa
Robert Houdek
At-Large
Stuart A. Cohen
Conventional Military Issues
John Landry
East Asia
Arthur Brown
Economics & Global Issues
Karen Monaghan
ActingEurope
Barry F. Lowenkron
Latin America
Fulton T. Armstrong
Near East and South Asia
Paul Pillar
Russia and Eurasia
George Kolt
Science & Technology
Lawrence Gershwin
Strategic & Nuclear Programs
Robert D Walpole
Warning
Robert Vickers
[1] These estimates reflect the expected number of HIV and AIDS cases at that time—not a cumulative total of all cases over the entire period.
[2] Although the lethal human immunodeficiency virus (HIV-1) was not characterized until the early 1980s, blood samples from Sub-Saharan Africa in the 1950s and 1960s have been tested retrospectively and found to be HIV-positive.
[3] Prevalence refers to the total number of people infected as a percentage of the adult (ages 15 to 49) population.
[4] Anand K Pandav, CS and Nath LM: The Impact of HIV/AIDS on the National Economy of India. Health Policy 47 (1999) pps 195-205. The costs of antiretroviral therapy, retraining the work force, strengthening the healthcare system, R&D, communications and prevention of mother-to-child transmission were not included in this model.